Introduction: Ethical Tensions in Gender-Affirming Care
I sit across from Evan (pseudonym), a fourteen-year-old transmasculine student, as he struggles through tears to find his words. His shoulders are tense, his gaze fixed downward. Like many trans and gender nonconforming (TGNC) youth, Evan faces family rejection and systemic invalidation, presenting with depression, anxiety, and disordered eating, all integrally intertwined with gender dysphoria. After being hospitalized for low body weight, he was enrolled in an eating disorder recovery program but was withdrawn by his parents after the physician suggested gender-affirming care. With puberty progressing and Evan’s chest beginning to develop, his food restriction has intensified, and he reports counting calories with increasing frequency.
After a long silence, Evan finally musters the courage to ask, “Would you be willing to get me a chest binder?” He is asking for a simple piece of cloth; something that, if he identified with his sex-assigned-at-birth, might be given without question in the form of a sports bra. Yet within this context, the request becomes ethically and institutionally complex. Every internal instinct in me responds immediately: yes, of course. Through Self Psychology (Kohut, 1977) and my lived experience, I understand that access to a binder is not merely material, but a selfobject experience that supports a more cohesive and livable sense of self. Yet, the deontological boundaries reinforced through social work education, shaped by risk- and litigation-averse frameworks and reflected in prevailing interpretations of the NASW Code of Ethics, suggest that doing so could be viewed as professionally inappropriate, ethically questionable, or even dangerous to my career (Reamer, 2013; Sinclair et al., 2023; Woodcock, 2011).
Evan’s experience is not an isolated one; TGNC youth experience disproportionately high rates of depression, suicidality, family rejection, and housing instability due to cultural transphobia operating across all ecological levels (Nath et al., 2024; Ryan et al., 2009, 2010, 2013, 2023; Toomey et al., 2010, 2018). These outcomes reflect broader conditions of relational deprivation, a chronic failure of recognition, affirmation, and belonging at scale. In response, queer and trans communities have long developed alternative systems of care, including chosen family structures, ballroom houses, and intergenerational networks of trans “mothers” and “fathers,” which provide both emotional support and material resources in contexts where traditional systems have failed (Arnold & Bailey, 2009; Burningham & Weiler, 2021; Kim & Feyissa, 2021; Perone et al., 2025; Telander et al., 2017). Within these communities, mutual aid practices, such as the sharing of clothing, housing, and gender-affirming medical resources like hormones, reflect an understanding that care must be collectively generated in the absence of institutional support (Breder & Bockting, 2025; Joseph & Bain, 2024; Matarese et al., 2024; Morgan, 2025; Webb, 2025).
From a developmental perspective, these varying forms of care are not secondary, they’re essential. Self Psychology posits that throughout childhood and adolescence, a cohesive sense of self emerges through core selfobject experiences of mirroring, idealization, and twinship (Kohut, 1977). For TGNC youth, these experiences are often disrupted or entirely absent within the family-of-origin and broader social environments (Hendricks & Testa, 2012; Meyer, 2003; Russell et al., 2007; Ryan et al., 2009, 2010, 2013, 2023). In this context, affirming adults in schools, clinics, and youth-serving organizations may step in as critical sources of these selfobject functions, offering recognition, stability, and the possibility of a livable future (Ancheta et al., 2021; Dessel et al., 2017; Wright, 2021).
At the same time, these community-based forms of care often exist in tension with dominant professional and ethical frameworks within social work and related fields. Institutional guidelines, including those reflected in the NASW Code of Ethics, prioritize clear role boundaries, risk management, and the avoidance of dual relationships (Doel et al., 2010; Reamer, 2018). Although important and intended to safeguard against harm, many scholars argue these frameworks reflect standardized assumptions about care that do not fully account for relational context, cultural practice, or structural inequities (Chu & Tsui, 2008; Chu et al., 2009; Gray, 2010; O’Leary et al., 2013). Within TGNC communities, this tension is further shaped by broader systems of cissexism and cisgenderism, described as a pervasive ideology among psychology that pathologizes TGNC identities (Ansara & Hegarty, 2011). Degtiar et al. (2025) extend this to demonstrate how structural cissexism produces measurable disparities in access to preventive all forms of care.
Evan’s request for a binder brings this tension into sharp focus. Is providing or facilitating access to this gender-affirming resource an ethical boundary violation, or a necessary act of care? What does it mean to uphold professional ethics in a context where traditional support systems have already failed? And how might social work more fully account for the relational and material realities that shape the lives of TGNC youth? This paper argues that rigid interpretations of professional boundaries within clinical social work, including those shaped by the NASW Code of Ethics, are insufficient for addressing the needs of TGNC youth. Drawing on Self Psychology, Minority Stress Theory, and scholarship on chosen family, practice wisdom, and clinical judgment, this paper begins to develop a Relational Ethics Framework for Clinical Judgment in Gender-Affirming Care that distinguishes exploitative boundary violations from contextually responsive, developmentally supportive forms of care. In doing so, this paper aims to contribute to a more nuanced understanding of ethical practice, one that remains accountable to professional standards while also responsive to the lived realities of TGNC youth.
A Review of the Literature
Dominant approaches to ethics in social work prioritize clear boundaries, professional distance, and risk management. In practice, however, these frameworks often fall short in addressing the realities faced by TGNC youth, whose lives are shaped by systemic marginalization and unmet relational needs. Research across cultural transphobia, developmental theory, chosen family, and professional ethics reveals a consistent tension between institutional models of care and the forms of support required in these contexts. This tension underscores the need to reconsider how ethical practice is understood and enacted.
TGNC Youth & Cultural Transphobia
TGNC youth face markedly elevated risks compared to their cisgender peers, with 46% more likely to consider suicide and 65% reporting experiences of discrimination (Johns et al., 2019, 2020; Nath et al., 2024). For TGNC youth, this trend reflects cultural transphobia operating across micro, meso, and macro-level systems, within homes, communities, and institutions. At the macro level, in 2026, over seven-hundred active anti-LGBTQ+ legislative bills are being considered across forty-two states (Trans Legislation Tracker, 2026), with states enacting laws like Florida House Bill 1557 (2022), the Parental Rights in Education Act, which legally restricts classroom discussions on gender and sexuality. As of early 2026, over twenty-five states have enacted laws or regulations that restrict transgender youth from participating in school sports that align with their gender identity, primarily targeting transgender girls from competing on female sports teams (Trans Legislation Tracker, 2026).
Erni (2012, 2016) argued that such laws codify transphobia by regulating gender recognition and punishing gender variance. Erni (2016) expands this argument, showing how laws regulating gender recognition, such as name changes, documentation, or medical “proof” requirements, make trans people’s existence conditional on state approval, essentially criminalizing gender diversity. These findings illustrate how structural and cultural transphobia shape lived experience through intertwined systems of exclusion and control, reflecting what Miliora (2000) describes as a cultural empathic failure, or society’s inability to recognize and affirm marginalized identities, which parallels the intrapsychic empathic failures that disrupt individual development. Chronic exposure to transphobia at multiple ecological levels reinforces these empathic failures (Miliora, 2000), making affirming relationships not just therapeutic but reparative.
Nath et al. (2024) demonstrated that parental acceptance of gender identity was associated with 36% lower odds of a suicide attempt among TGNC youth of color, underscoring that affirmation is not merely supportive but lifesaving. Relationships beyond the family can also help to repair family-of-origin failures. Hidalgo et al. (2019) found that peer affirmation and community connectedness significantly buffered the effects of minority stress, while Toomey et al. (2010, 2018) and Ancheta et al. (2021) showed that affirming social climates increased protective factors such as feelings of self-worth and belonging. Dessel et al. (2017) found that teacher support significantly increased school belonging and reduced depressive symptoms among LGBTQ+ students, with particularly strong effects for TGNC youth, demonstrating the importance of these relational environments.
Protective factors like chosen family networks then function as community-based selfobjects, offering the mirroring, idealization, and twinship absent in unsupportive families-of-origin (Goldstein, 2001; Kohut, 1977; Miliora, 2000). I argue that when TGNC clinicians model the warmth and affirmation characteristic of elder mentors and chosen family within professional boundaries, they provide corrective emotional experiences, offering the empathic attunement necessary to restore self-cohesion (Goldstein, 2001; Kohut, 1977; Miliora, 2000). In this way, clinical ethics and queer legacy aren’t oppositional; they can be integrated into a relational model that emphasizes responsiveness, mutuality, and care (Morgan, 2025; O’Leary et al., 2013).
Self Psychology & Minority Stress Theory
Heinz Kohut’s (1977) Self Psychology offers a developmental framework for understanding how early experiences of empathy, affirmation, and recognition shape a cohesive sense of self. Central to this theory is the concept of selfobjects, people, experiences, and relationships that fulfill essential psychological functions across development (Kohut, 1977). Kohut identified three core selfobject needs: mirroring (the experience of being validated), idealization (connection to stable role models), and twinship (a sense of belonging). When these needs are consistently met, they support what Kohut describes as healthy narcissism, or a stable sense of self-worth and confidence.
When these needs go unmet, however, individuals experience what Kohut (1977) termed empathic failure, which can result in fragmentation of the self and persistent feelings of shame and insecurity. In environments of repeated invalidation or rejection, these disruptions may take the form of what Miliora (2000) conceptualizes as narcissistic trauma, an injury to the developing self, caused by chronic failures of recognition. Extending this framework, Miliora (2000) and Whitsett and Whitsett (1996) argue that systemic forms of oppression, such as racism, operate as collective empathic failures that shape identity development at a structural level. Building on this scholarship, cultural transphobia can be understood as functioning in similar ways, producing widespread and cumulative disruptions to the development of a cohesive self among TGNC youth.
Minority Stress Theory (MST) complements this developmental perspective by identifying the social conditions that create these disruptions. Meyer (2003) conceptualizes minority stress as a chronic process stemming from stigma, prejudice, and discrimination, operating across both distal (external) and proximal (internalized) levels. Subsequent adaptations of MST for TGNC populations highlight how these stressors are compounded by structural barriers, including healthcare discrimination, legal misrecognition, and exclusion from public spaces (Hendricks & Testa, 2012). Empirical research further demonstrates how these conditions contribute to heightened psychological distress, internalized stigma, and diminished sense of belonging among TGNC youth (Ansara & Hegarty, 2011; Bauer et al., 2009; Blyth & McRae, 2018; Hidalgo et al., 2019; Nath et al., 2024; Toomey et al., 2010, 2018).
Within this struggle, the absence of affirming relationships is central. For TGNC youth living in rejecting family systems, navigating unsafe school climates, or experiencing the broader anti-trans movements, opportunities for mirroring, idealization, and twinship are often limited or entirely absent. Through Self Psychology, Wright (2021) suggests that the counselor can function as a reparative selfobject, meeting unmet developmental needs through consistent, attuned interactions within the therapeutic relationship. Applying self-psychological principles to micro-interactions, the counselor uses clinical judgment to choose a response (in both verbal and nonverbal ways) based on what the client needs: to feel better (via affirming mirroring), to feel seen (via empathic twinship), or to feel explicitly helped (via a guiding idealized adult). These moments, while often small, can provide critical experiences of recognition, stability, and belonging that support psychological integration.
Together, Self Psychology and Minority Stress Theory provide a complementary framework for understanding both the developmental impact of unmet interpersonal needs and the structural conditions that produce them. When integrated with scholarship on chosen family and mutual aid (Arnold & Bailey, 2009; Blair & Pukall, 2015; Burningham & Weiler, 2021; Huynh, 2023; Jackson Levin et al., 2020; Kim & Feyissa, 2021; Knauer, 2016; Matarese et al., 2024; Milton & Knutson, 2023; Morgan, 2025; Perone et al., 2025; Telander et al., 2017; Webb, 2025), this body of work highlights the central role of affirming relationships in mitigating trauma and supporting development among TGNC youth.
Chosen Family & Mutual Aid
Queer and trans communities have long developed alternative systems of care in response to the persistent failures of families, schools, medical institutions, and governments (Arnold & Bailey, 2009; Blair & Pukall, 2015; Burningham & Weiler, 2021; Huynh, 2023; Jackson Levin et al., 2020; Kim & Feyissa, 2021; Knauer, 2016; Matarese et al., 2024; Milton & Knutson, 2023; Morgan, 2025; Perone et al., 2025; Telander et al., 2017; Webb, 2025). Scholarship on chosen family and queer kinship consistently demonstrates that LGBTQ+ individuals, particularly those rejected by families-of-origin, construct relational networks that provide emotional, social, and material support outside of traditional institutional structures (Knauer, 2016; Huynh, 2023; Morgan, 2025). These networks function not only as sites of belonging but as critical infrastructures of survival and resistance.
Research on ballroom culture further illustrates how these systems operate in practice. Within house structures led by older “mothers” and “fathers,” Black and Latinx queer and trans youth, most of whom experienced homelessness or family rejection, received care, affirmation, and love (Arnold & Bailey, 2009; Telander et al., 2017; Joseph & Bain, 2024). These forms of chosen family provide essential selfobject functions and have been described as life-sustaining, particularly in contexts where structural and familial systems fail to meet basic developmental needs.
Contemporary research suggests that these relational systems persist across the life course and often take on intergenerational forms. Studies of LGBTQ+ communities document how older adults frequently act as mentors, caregivers, and cultural anchors for younger members, creating ongoing networks of mutual support (Breder & Bockting, 2025; Perone et al., 2025). Empirical work on natural mentoring further supports the protective function of these relationships, with findings indicating that mentorship, particularly when grounded in shared lived experience, can buffer the effects of minority stress among LGBTQ+ youth (Burningham & Weiler, 2021). Similarly, Kim and Feyissa’s (2021) conceptualization of chosen family as queer kinship emphasizes that these relational formations emerge in direct response to the absence or unsafety of biological family systems, necessitating flexibility, role overlap, and mutuality.
These findings have important implications for how care is understood and practiced within formal helping professions. Within social work, training emphasizes maintaining professional distance, avoiding dual relationships, and limiting the provision of material support (Doel et al., 2010; Reamer, 2018). While these guidelines are essential in preventing exploitation, their universal application can constrain responsiveness in contexts where clients’ interpersonal and material needs are deeply intertwined (Gray, 2010; O’Leary et al., 2013). Boundary crossings may be interpreted as inherently problematic, rather than evaluated in relation to intent, context, and developmental need (Alexander & Charles, 2009; Kapelj, 2022). For TGNC youth experiencing chronic invalidation or lack of familial support, this rigidity can restrict access to forms of care that are both developmentally protective and culturally grounded in queer and trans survival practices (Arnold & Bailey, 2009; Burningham & Weiler, 2021; Kim & Feyissa, 2021; Jackson Levin et al., 2020).
Collectively, this body of literature begins to highlight a critical disconnect between institutional models of ethical practice and the relational realities of queer and trans communities. While professional training emphasizes strict boundary maintenance, LGBTQ+ community survival has historically depended on boundary flexibility, mutual aid, and interdependent care (Morgan, 2025). This tension raises important questions for social work practice: how can clinicians ethically engage in culturally grounded forms of care without violating professional standards? And to what extent must those standards evolve to adequately meet the needs of TGNC youth?
Shared Identity in the Therapeutic Relationship
Navigating predominantly cisheteronormative environments, one of the main contributors to poor mental health among TGNC youth is isolation (Jayaratne et al., 2002; Johns et al., 2019, 2020; Nath et al., 2024). Without easy access to community or TGNC role models, youth lack consistent opportunities for affirmation, recognition, and a sense of belonging. Alternatively, relationships with TGNC adults offer a shared identity context that can shift how youth are seen and understood, often increasing the ease of recognition and relational attunement while reducing the burden of explaining or justifying one’s experience. Research suggests that shared identity within the dyad does not necessarily determine treatment outcomes; however, it plays a meaningful role in shaping how the relationship develops, particularly in fostering trust, validation, and a sense of being understood (Aladdin, 2008; Atkinson et al., 1984; Aymer, 2016; Cabral, 2011; Jayaratne et al., 2002; Thompson & Alexander, 2006).
Aymer (2016) shows how shared lived experience between clinician and client can deepen empathic attunement, support validation of race-based trauma, and build trust within the therapeutic relationship. Drawing on his own experiences as a Black man, the clinician reframes the client’s distress as a response to systemic racial oppression rather than individual pathology, enabling deeper engagement and more meaningful interpretation. Similarly, Thompson & Alexander (2006) found that while racial matching alone did not significantly impact outcomes, clients disclosed more deeply and were more willing to continue treatment longer.
These findings suggest that while shared identity supports relational elements, it is the active recognition and integration of lived experience within the therapeutic process that most strongly shapes the work. This means any cisgender clinician can learn to work with these unmet needs, but when we consider the long history of chosen family in queer and trans communities, the dynamic shifts. When the counselor themself is TGNC, the potential impact of those micro-interactions is amplified; they carry the weight of lived experience, lineage, and identification that many TGNC youth rarely receive elsewhere.
For example, a cis clinician may be able to empathize with and affirm a TGNC client experiencing gender dysphoria. However, a TGNC clinician may draw on lived experience of having navigated and survived similar challenges, allowing them to function as an affirming mirror, an understanding twin, and an idealized figure within the relationship. Through thoughtful and intentional disclosure, the clinician may deepen a sense of shared experience, supporting twinship and recognition. At the same time, their presence as someone who has moved through similar struggles can offer an idealizing function, helping the client imagine what is possible for their own future. Unfortunately, the lack of TGNC providers remains significant, as does the absence of gender and sexuality education within MSW curricula (Velez et al., 2023). Without adequate training, cishetero clinicians may feel uncertain about how to navigate gender-affirming practice in ethically and professionally grounded ways.
NASW Code of Ethics & Professional Culture
In tracing the origins of the NASW Code of Ethics, scholars have shown that the rise of biomedical, applied, and legal professional ethics in the 1980s, driven largely by increasing litigation across the helping professions, significantly shaped the Code’s development (Cnossen & Pearce, 2020; O’Leary et al., 2013; Ramsay, 2003; Reamer, 2018; Woodcock, 2011). O’Leary et al. (2013) link the Code’s risk-averse professional boundary expectations to medical models with strict hierarchies, arguing that this rigidity conflicts with core social work values such as relationality, social justice, cultural humility, and intersubjectivity. Similarly, Chu et al. (2008, 2009) and Kapelj (2022) highlight how traditional boundary frameworks position the clinician as an authoritative expert, rather than as a collaborator engaged in shared meaning-making. This hierarchical positioning has been widely critiqued for privileging objectivity, separation, and professional authority (Tower, 1994; Warshaw, 1989), yet despite these critiques, the model continues to shape how boundaries are conceptualized and enforced within social work (Ramsay, 2003).
Within this paradigm, professional boundaries are often framed through metaphors of separation. “Crossing the line” or “blurring boundaries” suggests that ethical practice depends on maintaining clear distinctions between worker and client. Sinclair et al. (2023) critique the personal/professional dichotomy as undermining relational connection, proposing instead that boundaries be understood as continuously enacted rather than fixed or transgressed. As Pugh (2007) demonstrates in the context of rural social work, such clear separations are often difficult to maintain in practice, with overlapping roles and community visibility making dual and multiple relationships unavoidable. Given the interconnected nature of many LGBTQ+ communities, clinicians and clients may be more likely to encounter similar overlapping social networks and spaces.
In practice, these professional boundaries are largely universalized, even though the realities of social work and our clients are diverse and context-specific (Anderson & Wiggins-Carter, 2004; Sudbery, 2002). The assumption that objectivity is achieved through distance overlooks the inherently relational and intersubjective nature of social work encounters (Ward et al., 2018). A growing body of relational and postmodern scholarship challenges the adequacy of these boundary models, arguing that strict separation between practitioner and client is often incompatible with context-sensitive, client-centered practice (Alexander & Charles, 2009; Chu & Tsui, 2008; Collins, 2020; Doel et al., 2010; Gray, 2010; O’Leary et al., 2013; Sinclair, 2023). Instead, these scholars advocate for boundary frameworks that emphasize mutuality, negotiation, and responsiveness. Within this view, boundaries are not fixed rules but evolving aspects of the relationship, requiring ongoing ethical reflection.
Kagle and Giebelhausen (1994) offer an important distinction between boundary violations, which are exploitative and harmful, and boundary crossings, which may be contextually appropriate and therapeutically beneficial. This distinction shifts ethical attention away from whether a professional norm has been crossed and toward the intent and potential impact of the action itself. However, while this distinction is useful conceptually, it provides less guidance regarding how clinicians determine whether an action constitutes a crossing or a violation in complex practice situations. I argue that making this determination requires broader consideration of developmental, relational, cultural, and structural contexts, which informs the proposed relational ethics framework.
Reviewing organizational context, Ward et al. (2018) argue that boundary rigidity often emerges as a defensive practice within risk-averse institutions, like schools, where anxiety about liability and harm is managed through control. In such environments, strict boundaries may function less as an ethical necessity and more as a strategy for managing uncertainty. Warshaw (2015) shows how overly fixed structures can inadvertently reproduce dynamics of control and disempowerment when working with marginalized communities, such as victims of domestic violence. These insights suggest that boundary practices cannot be understood solely as ethical safety nets but must also be examined in relation to institutional systems of power.
At the broader level, scholars have also critiqued the global dissemination of Western boundary frameworks. Ethical standards developed within Euro-American contexts have been widely adopted internationally, including by the Australian Association of Social Workers (2010), the British Association of Social Workers (2014), and the Hong Kong Social Workers Registration Board (2009). O’Leary et al. (2013) argue that this globalization risks imposing culturally specific norms as universal standards, while Chu et al. (2008, 2009) highlight how such approaches may overlook local relational practices and ethical traditions. Gollan and O’Leary (2009) further emphasize that social work practice is shaped by histories of power, colonization, and inequality, calling for greater accountability to cultural context in ethical decision-making.
Within the United States, Jayaratne et al. (2002) explored differences in how social workers from diverse racial backgrounds perceived the appropriateness of professional behaviors, and argued that practitioners may experience tension between the norms of the profession and the cultural values and identities they bring to practice.
If the perceived disparity is high, and an individual places greater value on identity with personal culture, they may choose to belong to a professional group which they perceive is more closely allied with that culture. For example, the National Association of Black Social Workers Statement of Purpose notes: “While the social work profession supposedly deals with the common human needs of all individuals, regardless of race or ethnic origin, we have found that there are needs peculiar to Black folk that have not been dealt with by the classic social work institutions and agencies” (National Association of Black Social Workers, 1982, p. i).
Our universalized professional ethics and boundaries stem from systems with a long-standing history of discrimination and oppression, so we must begin expanding authority across different forms of wisdom.
Across this body of literature, a consistent theme emerges – professional boundaries are not fixed or universal, but socially constructed, context-dependent, and shaped by relational, cultural, political, and institutional dynamics. Rather than functioning solely as risk-management tools, boundaries can be understood as negotiated aspects of practice that require reflexivity, attentiveness to power, and responsiveness to client needs (Gray, 2010; O’Leary et al., 2013). Navigating these boundaries demands active interpretation and decision-making in diverse, complex, and uncertain contexts, which is supported by practice wisdom and implemented through clinical judgment.
Practice Wisdom & Clinical Judgment
Practice wisdom is a topic within Western social work that has, until recent decades, received less attention than more empirical models (Cheung, 2016, 2017; Chu & Tsui, 2008; Chu et al., 2009; Dybicz, 2004; Gray & Fook, 2004; Kitchener & Brenner, 1990; Klein & Bloom, 1995; Samson, 2015; Sheppard, 1995; Tsang, 2008). Across the literature, however, social work is increasingly understood not as a purely technical or rule-based profession, but one that requires ongoing interpretation and decision-making in complex, uncertain contexts (Chu & Tsui, 2008; Gray & Fook, 2004). Within this shift, ethical decision-making becomes a distinct challenge, requiring practitioners to actively weigh competing principles rather than rely on procedural guidance alone (Cheung, 2016, 2017; Chu et al., 2009). This perspective is reinforced by broader critiques of technical-rational models, which argue that standardized approaches cannot adequately account for the variability and complexity of practice across contexts (Gray & Fook, 2004).
Within social work, this capacity for interpretation and context-sensitive decision-making is often described as practice wisdom. Although there is no single definition, consensus holds that practice wisdom extends beyond formal knowledge or procedural skill, encompassing the ability to draw on experience, values, and contextual awareness to respond effectively to unique situations (Chu & Tsui, 2008; Chu et al., 2009; Dybicz, 2004; Kitchener & Brenner, 1990; Klein & Bloom, 1995). It involves an ongoing process of reflection-in-action, in which practitioners recognize the limits of their knowledge, remain open to what they do not yet understand, and adjust their approach in situations where there is no clear or predefined solution (Dybicz, 2004). Broader discussions of wisdom further support this understanding, emphasizing the ability to make sound judgments under conditions of uncertainty, integrate multiple perspectives, and balance competing demands (Kitchener & Brenner, 1990).
Practice wisdom allows practitioners to identify nuance, recognize patterns that may not be captured in formal frameworks, and remain responsive to the relational and situational dynamics of each encounter (Chu & Tsui, 2008; Chu et al., 2009; Dybicz, 2004). It also involves staying aware of how one’s positionality, values, and assumptions shape perception and decision-making, making reflexivity central to how it’s applied. For newer clinicians, practice wisdom may be less developed through experience; however, those who share aspects of identity or lived experience with the communities they serve may draw on experiential knowledge that can deepen their understanding of clients’ realities.
Beyond wisdom derived from practice, it would be remiss not to also include the guiding knowledge gained from the lived experiences of marginalized communities. In their work centering Women of Color practice wisdom, Melendez, Ballesteros, and Jemal (2026) frame this knowledge as a form of epistemic disobedience, or a refusal to conform to dominant ways of knowing and validating knowledge. In this context, epistemic disobedience involves reclaiming lived experience, historical context, and cultural standpoint as legitimate sources of knowledge production, particularly within systems that have historically marginalized or excluded these perspectives (Melendez et al., 2026).
Importantly, the authors caution against equating lived experience alone with expertise, emphasizing instead that practice wisdom emerges through the process of navigating, interpreting, and responding to systems of power (Melendez et al., 2026). As such, this perspective does not position lived experience as a replacement for formal knowledge, but as a critical expansion of what counts as knowledge in practice. In applied contexts, this form of wisdom is often reflected in community-based models of care, such as recovery communities, peer-support programs, and mutual aid networks, where experiential knowledge is treated as a vital resource for understanding and responding to complex human needs. With this expanded understanding of knowledge, the challenge then shifts to how they are brought together in practice.
If practice wisdom reflects what clinicians draw upon, clinical judgment is the process through which it is applied in practice (Chu & Tsui, 2008; Chu et al., 2009; Clark, 2006; Kitchener & Brenner, 1990). Clinical judgment can be understood as the process through which ethical principles are interpreted and enacted in context. It involves integrating practice wisdom, professional knowledge, experience, values, and situational awareness to determine what constitutes an appropriate response in each given moment. In this sense, clinical judgment can also be understood as a site of epistemic negotiation, where practitioners weigh dominant institutional expectations against relational, experiential, and contextual forms of knowledge (Melendez et al., 2026). This process requires not only technical competence but also the capacity to recognize the limits of standardized frameworks and to act in ways that are responsive to the realities of clients’ lives. Particularly in work with marginalized populations, clinical judgment may involve drawing on forms of knowledge that are not formally recognized within institutional settings yet are essential to ethical and effective practice (Melendez et al., 2026).
This emphasis on clinical judgment is further supported by relational and context-oriented approaches to social work practice. Boundaries are increasingly understood as fluid, negotiated, and shaped by relational and situational dynamics rather than fixed rules (Doel et al., 2010; Grant & Mandell, 2016; Kagle & Giebelhausen, 1994; Kapelj, 2022; O’Leary et al., 2013; Pugh, 2007; Shevellar & Barringham, 2016; Sinclair et al., 2023). As a result, practitioners must continuously interpret and adapt ethical principles within specific contexts, rather than rely solely on procedural guidance. This aligns with broader arguments that ethical practice requires ongoing reflexivity, dialogue, and responsiveness to client needs (Gray & Fook, 2004; Shevellar & Barringham, 2016). Taken together, these perspectives suggest that ethical practice is not achieved through strict adherence to rules alone, but through the thoughtful and reflexive use of clinical judgment.
Toward a Relational Ethics Framework in Practice
Coady (1993) documents how the profession’s historical emphasis on the worker–client relationship has been overshadowed by increasing focus on technique and scientific legitimacy, despite evidence that relational factors remain the primary drivers of outcomes. Similarly, relationship-based approaches to practice emphasize that meaningful change occurs within the context of human connection, where trust, collaboration, and emotional presence are central (Ward et al., 2018). From a service user perspective, Beresford et al. (2008) found that clients consistently value warmth, empathy, and relational authenticity, at times describing effective social work relationships in terms of “friendship.” These findings highlight a persistent tension between the relational qualities clients experience as helpful and the more procedural, distanced forms of professionalism emphasized in policy and training.
Although the field of social work has sought legitimacy through empirical science, the literature reviewed provides a perspective that client work is fundamentally judgment-based rather than technical-rational (Cheung, 2016, 2017; Chu & Tsui, 2008; Chu et al., 2009; Dybicz, 2004; Gray & Fook, 2004; Kitchener & Brenner, 1990; Klein & Bloom, 1995; Samson, 2015; Sheppard, 1995; Tsang, 2008). When a clinician is presented with a client challenge that is clear and for which there are evidence-based treatments, they can systematically apply the interventions. Often, however, clinicians are confronted by a condition that differs greatly from experiences reflected in the professional knowledge base. Klein and Bloom (1995) argue that when practitioners encounter such situations, they must draw on experience and contextual understanding to develop an appropriate response.
The literature, therefore, points to a necessary shift in how ethical practice is understood. When decision-making in practice is inherently context-dependent and grounded in judgment, ethical frameworks must account for this complexity. Professional boundaries, rather than functioning as fixed rules, are often fluid and relationally negotiated, and clinical judgment becomes the mechanism through which ethical principles are enacted. Ethical decision-making, therefore, cannot be reduced to rule adherence alone, but must be understood as a process of applied judgment, requiring practitioners to interpret ethical principles in relation to developmental need, relational context, and structural constraints (Chu & Tsui, 2008; Chu et al., 2009; Clark, 2006; Glebova et al., 2025; Gray & Fook, 2004).
In response, this section proposes a Relational Ethics Framework for Clinical Judgment in Gender-Affirming Care to guide clinical decision-making in work with TGNC youth. Although developed in the context of TGNC youth, this framework’s emphasis on relational responsiveness, clinical judgment, and contextual awareness holds broader applicability to work with marginalized populations whose needs are shaped by structural inequities and gaps in traditional systems of care. This framework offers a way to operationalize ethical decision-making practice by clarifying the considerations that shape how practitioners translate understanding into action.
As shown in Figure 1, the CARE Framework: Contextual Assessment for Relational Ethics Guiding Clinical Judgment in Gender-Affirming Care, ethical decision-making is guided by the interaction between practice wisdom, clinical judgment, and a set of five relational Decision Domains, illustrating how practitioners move from interpretation to action within complex, real-world contexts. This model does not replace existing ethical standards, but builds upon them, offering a way to distinguish between harmful boundary violations and contextually responsive, developmentally supportive boundary crossings. Grounded in practice wisdom and enacted through clinical judgment, it provides a structured yet flexible approach to navigating ethical complexity in real-world contexts (Dybicz, 2004; Kitchener & Brenner, 1990).
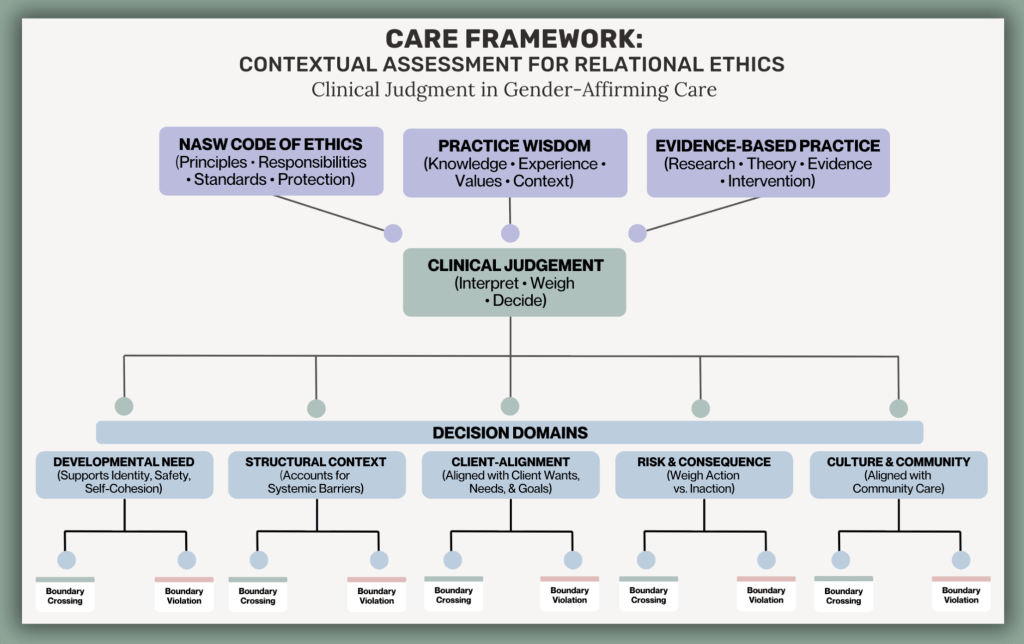
Figure 1. CARE Framework: Contextual Assessment for Relational Ethics Guiding Clinical Judgment in Gender-Affirming Care
Central to this framework is the distinction made by Kagle & Giebelhausen (1994) between boundary violations and boundary crossings. Boundary violations are actions that are exploitative, harmful, or primarily serve the needs of the practitioner, often resulting in a misuse of power. In contrast, boundary crossings are intentional, contextually responsive deviations from standard professional norms that are undertaken to meet a client’s needs and support therapeutic goals. This distinction shifts the focus from whether a boundary has been crossed to how and why the action occurred, requiring careful consideration of intent, impact, and context (Alexander & Charles, 2009; Kagle & Giebelhausen, 1994).
Within this framework, ethical decision-making is guided by five interrelated Decision Domains. First, Developmental Need considers whether an intervention supports the client’s psychological and emotional development. For TGNC youth, this includes access to affirming experiences that provide mirroring, idealization, and twinship, which are essential for the development of a cohesive sense of self (Kohut, 1977; Miliora, 2000). Second, Structural Context examines the broader systems shaping the client’s access to care, including experiences of marginalization, family rejection, and institutional barriers (Meyer, 2003; Hendricks & Testa, 2012).
Third, Client-Alignment grounds the collaborative intention behind the intervention, asking whether the action is clearly in service of the client’s wants, needs, and expressed goals, and whether the client is meaningfully included in shaping the outcome. Fourth, Risk and Consequence require an assessment not only of the potential risks of acting, but also of the risks of not acting, particularly in contexts where unmet needs contribute to psychological harm (Kitchener & Brenner, 1990). Fifth, Cultural and Community Context considers whether the intervention aligns with the relational norms and care practices of the client’s community (Burningham & Weiler, 2021; Jayaratne et al., 2002; Kim & Feyissa, 2021; Morgan, 2025).
Applying this framework to Evan’s request for a chest binder illustrates how clinical judgment is used to weigh multiple Decision Domains in practice. The request reflects a clear Developmental Need, directly tied to gender affirmation and the formation of a cohesive sense of self (Kohut, 1977). Within the Structural Context domain, access to affirming resources has been actively restricted by both family and medical systems, leaving Ethan without viable alternatives. The intent of providing a binder is explicitly Client-Aligned, and within the Risk and Consequence domain, the potential risks are minimal when weighed against the psychological and physical harm of ongoing dysphoria and disordered eating (Hendricks & Testa, 2012). Finally, within the Cultural and Community Context domain, providing access to a binder reflects LGBTQ+ care practices rooted in chosen family and mutual aid. Within this context, such an action is best understood not as a boundary violation but as a developmentally responsive and ethically grounded boundary crossing (Kagle & Giebelhausen, 1994).
Applying the framework to boundary decisions across different contexts further illustrates how intent, impact, and relational dynamics shape whether an action constitutes a crossing or a violation. For example, within the Developmental Need domain, consistently using a client’s chosen name and pronouns despite parental disapproval may function as a boundary crossing when it affirms identity and supports psychological safety. In contrast, disclosing a client’s chosen name or gender identity without their consent in order to satisfy institutional or parental demands would constitute a boundary violation, as it breaches confidentiality, undermines trust, and reflects a misuse of professional power. Here, the Structural Context domain is central, as the ethical complexity emerges from competing institutional and familial pressures that shape what can be disclosed and to whom.
The distinction between a boundary crossing and a boundary violation is also shaped by the Client-Alignment domain, particularly related to whose needs the intervention is serving. A TGNC clinician may engage in limited and intentional self-disclosure to support identification and shared understanding, strengthening the therapeutic relationship; however, disclosure that serves the clinician’s emotional needs or shifts the focus of care toward the clinician would constitute a boundary violation, as it disrupts relational balance and misuses the therapeutic space. Finally, informed by the Risk and Consequence domain, responding to a client outside of scheduled sessions during a moment of acute distress may represent a boundary crossing when it is time-limited, clinically justified, and grounded in client safety. Whereas unlimited availability that fosters dependency or meets the clinician’s desire to feel needed would be considered a boundary violation, as it blurs professional roles and reinforces an unhealthy power dynamic. Within the Cultural and Community Context domain, connecting a client to peer support or community-based resources outside of school may function as a boundary crossing, whereas dismissing or restricting these supports in favor of traditional or institutional options constitutes a boundary violation, as it disregards the client’s cultural context and limits access to meaningful care (Jayaratne et al., 2002; Kagle & Giebelhausen, 1994).
This framework does not suggest abandoning professional boundaries, but rather interpreting them as flexible and context-dependent elements of practice that require ongoing reflection. Ethical practice, in this sense, is not achieved through rigid compliance to rules, but through the careful exercise of clinical judgment grounded in practice wisdom (Cheung, 2016, 2017; Chu & Tsui, 2008; Chu et al., 2009; Dybicz, 2004; Gray & Fook, 2004; Kitchener & Brenner, 1990; Klein & Bloom, 1995; Samson, 2015; Sheppard, 1995; Tsang, 2008). For TGNC youth, whose lives are shaped by structural exclusion and relational gaps, this approach allows social workers to remain both ethically accountable and meaningfully responsive.
Implications for Clinical Practice
The framework proposed in this paper has several implications for how ethical practice is understood and enacted within social work, particularly in work with TGNC youth. First, it challenges the assumption that ethical competence is demonstrated through strict adherence to professional boundaries. Instead, it positions ethical practice as a form of applied judgment, requiring practitioners to interpret ethical principles in relation to developmental need, relational context, and structural constraint. This shift moves ethics away from procedural compliance and toward a more reflexive and context-sensitive approach to decision-making (Clark, 2006; Gray & Fook, 2004).
Second, this framework calls for a reexamination of how risk is conceptualized within ethical practice. Traditional models often prioritize the prevention of boundary violations, emphasizing potential harm associated with practitioner action (Reamer, 2018). While this concern remains important, the findings presented here suggest that inaction can also produce harm, particularly for TGNC youth whose access to affirming resources is already constrained. Ethical decision-making, therefore, must account for both the risks of crossing boundaries and the risks of maintaining them, especially in contexts shaped by systemic marginalization (Hendricks & Testa, 2012; Meyer, 2003).
Third, these findings have implications for social work education and supervision. If clinical judgment is central to ethical practice, then training must move beyond rule-based instruction and create space for practitioners to engage with ambiguity, reflect on their own positionality, and develop the capacity to make contextually grounded decisions. This includes cultivating practice wisdom through experience, reflection, and dialogue, rather than relying solely on standardized ethical guidelines (Chu & Tsui, 2008; Chu et al., 2009; Dybicz, 2004). Supervision, in turn, becomes a critical site for ethical deliberation, where clinicians can explore the tensions inherent in boundary decisions and receive support in navigating complex situations.
Finally, this framework highlights the importance of aligning professional practice with the relational realities of the communities’ social workers serve. For TGNC youth, care often takes place within systems of chosen family, mutual aid, and community-based support that do not conform to traditional models of professional distance. Recognizing and respecting these relational forms of care allows social workers to engage more authentically and responsively, while still maintaining ethical accountability (Kim & Feyissa, 2021; Sinclair et al., 2023).
Conclusion
This paper has argued that rigid interpretations of professional boundaries within social work are insufficient for addressing the needs of TGNC youth. Drawing on Self Psychology, Minority Stress Theory, and relational approaches to ethics, it has shown how experiences of invalidation and structural marginalization shape both developmental outcomes and access to care. Within this context, traditional boundary frameworks, grounded in separation and risk management, can constrain the very forms of support that are most needed.
In response, this paper proposed the Relational Ethics Framework for Clinical Judgment in Gender-Affirming Care that distinguishes between harmful boundary violations and contextually responsive boundary crossings. Grounded in practice wisdom and enacted through clinical judgment, this framework offers a way to navigate ethical complexity without abandoning professional responsibility. Rather than positioning ethics as a fixed set of rules, it understands ethical practice as an ongoing process of interpretation, reflection, and action in context (Chu & Tsui, 2008; Chu et al., 2009; Kitchener & Brenner, 1990).
Ultimately, this approach reframes ethical practice as something that is not only about maintaining boundaries, but about making thoughtful, accountable decisions in relationship with clients. For TGNC youth, whose lives are shaped by gaps in affirmation and support, this shift has direct implications for their safety, development, and well-being. By centering relational clinical judgment, social work can move toward a model of practice that is both ethically grounded and meaningfully aligned with the realities of the populations it serves.
References:
Alexander, C., & Charles, G. (2009). Caring, Mutuality and Reciprocity in Social Worker—Client Relationships: Rethinking Principles of Practice. Journal of Social Work: JSW, 9(1), 5–22. https://doi.org/10.1177/1468017308098420
Alladin, W. J. (2008). Ethnic Matching in Counselling: How Important is it to Ethnically Match Clients and Counsellors? In S. Palmer (Ed.), Multicultural Counselling: A Reader (pp. 175–180). SAGE Publications Ltd. https://doi.org/10.4135/9781446219188.n15
Ancheta, A. J., Bruzzese, J. M., & Hughes, T. L. (2021). The impact of positive school climate on suicidality and mental health among LGBTQ adolescents: A systematic review. The Journal of School Nursing, 37(2), 75–86. https://doi.org/10.1177/1059840520970847
Anderson, J., & Wiggins-Carter, R. (2004). Diversity Perspectives for Social Work Practice. In Paradigms of Clinical Social Work (1st ed., Vol. 3, pp. 19–34). Routledge. https://doi.org/10.4324/9780203938010-4
Ansara, Y. G., & Hegarty, P. (2011). Cisgenderism in psychology: Pathologising and misgendering children from 1999 to 2008. Psychology & Sexuality, 3(2), 137–160. https://doi.org/10.1080/19419899.2011.576696
Arnold, E. A., & Bailey, M. M. (2009). Constructing Home and Family: How the Ballroom Community Supports African American GLBTQ Youth in the Face of HIV/AIDS. Journal of Gay & Lesbian Social Services, 21(2–3), 171–188. https://doi.org/10.1080/10538720902772006
Atkinson, D. R., Ponce, F. Q., & Martinez, F. M. (1984). Effects of ethnic, sex, and attitude similarity on counselor credibility. Journal of Counseling Psychology, 31(4), 588–590. https://doi.org/10.1037/0022-0167.31.4.588
Australian Association of Social Workers (AASW). (2010). Code of Ethics: Australian Association of Social Workers. Canberra, AASW
Aymer, S. R. (2016). “I can’t breathe”: A case study-Helping Black men cope with race-related trauma stemming from police killing and brutality. Journal of Human Behavior in the Social Environment, 26(3–4), 367–376. https://doi.org/10.1080/10911359.2015.1132828
Bauer, G. R., Hammond, R., Travers, R., Kaay, M., Hohenadel, K. M., & Boyce, M. (2009). “I Don’t Think This Is Theoretical; This Is Our Lives”: How Erasure Impacts Health Care for Transgender People. The Journal of the Association of Nurses in AIDS Care, 20(5), 348–361. https://doi.org/10.1016/j.jana.2009.07.004
.
Beresford, P., Croft, S., & Adshead, L. (2008). ‘We Don’t See Her as a Social Worker’: A Service User Case Study of the Importance of the Social Worker’s Relationship and Humanity. The British Journal of Social Work, 38(7), 1388–1407. https://doi.org/10.1093/bjsw/bcm043
Blair, K. L., & Pukall, C. F. (2015). Family matters, but sometimes chosen family matters more: Perceived social network influence in the dating decisions of same- and mixed-sex couples. The Canadian Journal of Human Sexuality, 24(3), 257–270. https://doi.org/10.3138/cjhs.243-A3
Blyth, C., & McRae, P. (2018). “Death by a Thousand Paper Cuts”: Transphobia, Symbolic Violence, and Conservative Christian Discourse. In Rape Culture, Gender Violence, and Religion: Interdisciplinary Perspectives (pp. 111-133). Cham: Springer International Publishing.
Breder, K., & Bockting, W. (2025). Examining LGBT older adult social networks and chosen families using the convoy model of social relations. Journal of Family Theory & Review, 17(2), 284–300. https://doi.org/10.1111/jftr.12609
British Association of Social Workers. (2014). The Code of Ethics for Social Work. Birmingham: BASW
Burningham, K. L., & Weiler, L. M. (2021). Natural Mentoring and LGBTQ Youth: A Systematic Review. Adolescent Research Review, 6(4), 391–407. https://doi.org/10.1007/s40894-020-00146-x
Cabral, R. R., & Smith, T. B. (2011). Racial/Ethnic Matching of Clients and Therapists in Mental Health Services: A Meta-Analytic Review of Preferences, Perceptions, and Outcomes. Journal of Counseling Psychology, 58(4), 537–554. https://doi.org/10.1037/a0025266
Cheung, J. C.-S. (2016). Researching Practice Wisdom in Social Work. Journal of Social Intervention, 25(3), 24–38. https://doi.org/10.18352/jsi.472
Cheung, J. C.-S. (2017). Practice wisdom in social work: an uncommon sense in the intersubjective encounter. European Journal of Social Work, 20(5), 619–629. https://doi.org/10.1080/13691457.2016.1255592
Chu, W. C. K., & Tsui, M. (2008). The nature of practice wisdom in social work revisited. International Social Work, 51(1), 47–54. https://doi.org/10.1177/0020872807083915
Chu, W. C. K., Tsui, M., & Yan, M. (2009). Social work as a moral and political practice. International Social Work, 52(3), 287–298. https://doi.org/10.1177/0020872808102064
Clark, C. (2006). Moral Character in Social Work. The British Journal of Social Work, 36(1), 75–89. https://doi.org/10.1093/bjsw/bch364
Cnossen, C. J. & Pearce, E. B. (2020). National Association of Social Workers Code of Ethics. In E. B. Pearce (Ed.), Introduction to Human Services. Open Oregon Educational Resources. Retrieved on 2/25/26 from: https://openoregon.pressbooks.pub/humanservices/chapter/nasw-code-of-ethics/
Coady, N. F. (1993). The Worker–Client Relationship Revisited. Families in Society: The Journal of Contemporary Social Services, 74(5), 291-300. https://doi.org/10.1177/104438949307400504
Degtiar, I., Kim, J., Michaels, E. K., Huff, I. R., Rudacille, M. E., Clusen, N. A., Ferguson, A., Smith-Howell, E. R., & Gonzales, G. (2025). Disparities in Preventive Health Services Between Transgender and Cisgender Adults by State-Level Policy Environments. American Journal of Preventive Medicine, 69(4), Article 107954. https://doi.org/10.1016/j.amepre.2025.107954
Dessel, A. B., Kulick, A., Wernick, L. J., & Sullivan, D. (2017). The importance of teacher support: Differential impacts by gender and sexuality. Journal of Adolescence, 56, 136–144. https://doi.org/10.1016/j.adolescence.2017.02.002
Doel, M., Allmark, P., Conway, P., Cowburn, M., Flynn, M., Nelson, P., & Tod, A. (2010). Professional boundaries: Crossing a line or entering the shadows? British Journal of Social Work, 40(6), 1866–1889. https://doi.org/10.1093/bjsw/bcq010
Doel, M. (2018). Service-user perspectives on relationships. In G. Ruch, D. Turney, & A. Ward (Eds.), Relationship-based social work: Getting to the heart of practice (2nd ed., pp. 199–213). Jessica Kingsley Publishers.
Dybicz, P. (2004). An Inquiry into Practice Wisdom. Families in Society, 85(2), 197–203. https://doi.org/10.1606/1044-3894.316
Erni, J. N. (2012). Legitimating transphobia: The legal disavowal of transgender rights in prison. Cultural Studies, 27(1), 136–159. https://doi.org/10.1080/09502386.2012.722305
Erni, J. N. (2016). Disrupting the colonial transgender/law nexus: Reading the case of W in Hong Kong. Cultural Studies ↔ Critical Methodologies, 16(4), 351–360. https://doi.org/10.1177/1532708616643987
Florida House Bill 1557, Parental Rights in Education Act, 2022 Regular Session. (2022). https://www.flsenate.gov/Session/Bill/2022/1557
Glebova, T., Lal, A., & Gangamma, R. (2025). Relational ethics in immigrant families: The contextual therapy five‐dimensional framework. Family Process, 64(1), e13071-n/a. https://doi.org/10.1111/famp.13071
Goldstein, E. (2001). Object Relations Theory and Self Psychology in Social Work Practice. NY: Free Press.
Gollan, S., & O’Leary, P. J. (2009). Teaching Culturally Competent Social Work Practice through Black and White Pedagogical Partnerships. Social Work Education, 28(7), 707–721. https://doi.org/10.1080/02615470802406502
Grant, J. G., & Mandell, D. (2016). Boundaries and relationships between service users and service providers in community mental health services. Social Work in Mental Health, 14(6), 696–713. https://doi.org/10.1080/15332985.2015.1137258
Gray, M. (2010). Moral sources and emergent ethical theories in social work. British Journal of Social Work, 40(6), 1794–1811. https://doi.org/10.1093/bjsw/bcp104
Gray, M., & Fook, J. (2004). The quest for a universal social work: some issues and implications. Social Work Education, 23(5), 625–644. https://doi.org/10.1080/0261547042000252334
Hendricks, M. L., & Testa, R. J. (2012). A Conceptual Framework for Clinical Work With Transgender and Gender Nonconforming Clients: An Adaptation of the Minority Stress Model. Professional Psychology, Research and Practice, 43(5), 460–467. https://doi.org/10.1037/a0029597
Hidalgo, M. A., Petras, H., Chen, D., & Chodzen, G. (2019). The gender minority stress and resilience measure: Psychometric validity of an adolescent extension. Clinical Practice in Pediatric Psychology, 7(3), 278–290. https://doi.org/10.1037/cpp0000297
Hong Kong Social Workers’ Registration Board. (2009). Code of Practice for Social Workers.
Huynh, J. (2023). “Family Is the Beginning but Not the End”: Intergenerational LGBTQ Chosen Family, Social Support, and Health in a Vietnamese American Community Organization. Journal of Homosexuality, 70(7), 1240–1262. https://doi.org/10.1080/00918369.2021.2018879
Jackson Levin, N., Kattari, S. K., Piellusch, E. K., & Watson, E. (2020). “We Just Take Care of Each Other”: Navigating ‘Chosen Family’ in the Context of Health, Illness, and the Mutual Provision of Care amongst Queer and Transgender Young Adults. International Journal of Environmental Research and Public Health, 17(19), 7346. https://doi.org/10.3390/ijerph17197346
Jayaratne, S., Croxton, T. A., & Mattison, D. (2002). Race, Practice Behaviors and the NASW Code of Ethics. Journal of Social Service Research, 28(3), 65–89. https://doi.org/10.1300/J079v28n03_04
Johns, M. M., Lowry, R., Andrzejewski, J., Barrios, L. C., Zewditu, D., McManus, T., et al. (2019). Transgender identity and experiences of violence victimization, substance use, suicide risk, and sexual risk behaviors among high school student–19 states and large urban school districts, 2017. Morbidity and Mortality Weekly Report, 68(3), 65–71. https://doi.org/10.15585/MMWR.MM6803A3
Johns, M. M., Lowry, R., Haderxhanaj, L. T., et al. (2020). Trends in violence victimization and suicide risk by sexual identity among high school students — Youth Risk Behavior Survey, United States, 2015–2019. Morbidity and Mortality Weekly Report, 69(Suppl-1), 19–27. https://doi.org/10.15585/mmwr.su6901a3
Joseph, J., & Bain, N. (2024). Leisure as black survival: ballroom, vogue, and black queer and trans+ embodied activism in Canada. Leisure (Waterloo), 48(2), 315–332. https://doi.org/10.1080/14927713.2024.2308911
Kagle, J. D., & Giebelhausen, P. N. (1994). Dual Relationships and Professional Boundaries. Social Work (New York), 39(2), 213–220. https://doi.org/10.1093/sw/39.2.213
Kapelj, A. (2022). Professional boundaries that promote dignity and rights in social work practice. Ethics and social welfare, 16(4), 450-456.
Kitchener, K. S., & Brenner, H. G. (1990). Wisdom and Reflective Judgment: Knowing in the Face of Uncertainty. In Wisdom: Its Nature, Origins, and Development, edited by Robert J. Sternberg, 212-227.
Kim, S., & Feyissa, I. F. (2021). Conceptualizing “Family” and the Role of “Chosen Family” within the LGBTQ+ Refugee Community: A Text Network Graph Analysis. Healthcare (Basel), 9(4), 369. https://doi.org/10.3390/healthcare9040369
Klein, W. C., & Bloom, M. (1995). Practice Wisdom. Social Work (New York), 40(6), 799–807. https://doi.org/10.1093/sw/40.6.799
Knauer, N. J. (2016). Lgbt Older Adults, Chosen Family, And Caregiving. The Journal of Law and Religion, 31(2), 150–168. https://doi.org/10.1017/jlr.2016.2
Kohut, H. (1977). The Restoration of the Self. Madison, CT: International Universities Press.
Matarese, M., Greeno, E., Weeks, A., Lorthridge, J., Hammond, P., & Deinhart, S. (2024). Building Connections Between Chosen Family and Kin: A Culturally Adapted Program for LGBTQ+ Children, Youth, and Their Families. Families in Society, 105(1), 81–93. https://doi.org/10.1177/10443894231204538
Melendez, D., Ballesteros, D., & Jemal, A. (2026). Honoring Women of Color Practice Wisdom as Epistemic Disobedience within Methods for Social Work Education Research. Journal of Teaching in Social Work, 46(1), 3–19. https://doi.org/10.1080/08841233.2025.2593661
Meyer, I. H. (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychological Bulletin, 129(5), 674-697. https://doi.org/10.1037/0033-2909.129.5.674
Mignolo, W. D. (2007). DELINKING: The rhetoric of modernity, the logic of coloniality and the grammar of de-coloniality. Cultural Studies (London, England), 21(2–3), 449–514. https://doi.org/10.1080/09502380601162647
Miliora, M. T. (2000). Beyond empathic failures: Cultural racism as narcissistic trauma and disenfranchisement of grandiosity. Clinical Social Work Journal, 28(1), 43–54. https://doi.org/10.1023/A:1005159624872
Milton, D. C., & Knutson, D. (2023). Family of Origin, Not Chosen Family, Predicts Psychological Health in a LGBTQ+ Sample. Psychology of Sexual Orientation and Gender Diversity, 10(2), 269–278. https://doi.org/10.1037/sgd0000531
Morgan, S. (2025). “We don’t tolerate each other; we actually respect and love each other”: Chosen family as a turning point among LGBTQ+ people. Criminology (Beverly Hills). https://doi.org/10.1111/1745-9125.70007
Nath, R., Matthews, D.D., DeChants, J.P., Hobaica, S., Clark, C.M., Taylor, A.B., & Muñoz, G. (2024). 2024 U.S. National Survey on the Mental Health of LGBTQ+ Young People. West Hollywood, California: The Trevor Project. Retrieved from https://www.thetrevorproject.org/survey-2024
O’Leary, P., Tsui, M.-S., & Ruch, G. (2013). The Boundaries of the Social Work Relationship Revisited: Towards a Connected, Inclusive and Dynamic Conceptualisation. The British Journal of Social Work, 43(1), 135–153. https://doi.org/10.1093/bjsw/bcr181
Perone, A. K., Toman, L., Glover Reed, B., Coldon, T., Osborne, A., & Cook, J. (2025). Aging and Mentorship in the Margins: Multigenerational Knowledge Transfer Among LGBTQ+ Chosen Families. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 80(6). https://doi.org/10.1093/geronb/gbaf027
Pugh, R. (2007). Dual Relationships: Personal and Professional Boundaries in Rural Social Work. The British Journal of Social Work, 37(8), 1405–1423. https://doi.org/10.1093/bjsw/bcl088
Ramsay, R. F. (2003). Transforming the Working Definition of Social Work into the 21st Century. Research on Social Work Practice, 13(3), 324–338. https://doi.org/10.1177/1049731503251976
Reamer, F. G. (1998). The evolution of social work ethics. Social work, 43(6), 488-500.
Reamer, F. G. (2018). Social Work Values and Ethics: An Overview. In Social Work Values and Ethics. Columbia University Press.
Russell, S. T., Ryan, C., Toomey, R. B., Diaz, R. M., & Sanchez, J. (2011). Lesbian, Gay, Bisexual, and Transgender Adolescent School Victimization: Implications for Young Adult Health and Adjustment. The Journal of School Health, 81(5), 223–230. https://doi.org/10.1111/j.1746-1561.2011.00583.x
Ryan, C. (2013). Generating a revolution in prevention, wellness, and care for LGBT children and youth. Temple Political & Civil Rights Law Review., 23.
Ryan, C., Barba, A., & Cohen, J. A. (2023). Family-Based Psychosocial Care for Transgender and Gender-Diverse Children and Youth. Child and Adolescent Psychiatric Clinics of North America, 32(4), 775–788. https://doi.org/10.1016/j.chc.2023.03.002
Ryan, C., Huebner, D., Diaz, R. M., & Sanchez, J. (2009). Family Rejection as a Predictor of Negative Health Outcomes in White and Latino Lesbian, Gay, and Bisexual Young Adults. Pediatrics (Evanston), 123(1), 346–352. https://doi.org/10.1542/peds.2007-3524
Ryan, C., Russell, S. T., Huebner, D., Diaz, R., & Sanchez, J. (2010). Family acceptance in adolescence and the health of LGBT young adults. Journal of Child and Adolescent Psychiatric Nursing, 23(4), 205–213. https://doi.org/10.1111/j.1744-6171.2010.00246.x
Samson, P. L. (2015). Practice wisdom: the art and science of social work. Journal of Social Work Practice, 29(2), 119–131. https://doi.org/10.1080/02650533.2014.922058
Sheppard, M. (1995). Social Work, Social Science and Practice Wisdom. The British Journal of Social Work, 25(3), 265–293. https://doi.org/10.1093/oxfordjournals.bjsw.a056180
Shevellar, L., & Barringham, N. (2016). Working in Complexity: Ethics and Boundaries in Community Work and Mental Health. Australian Social Work, 69(2), 181–193. https://doi.org/10.1080/0312407X.2015.1071861
Sinclair, A., Mahboub, L., Gillieatt, S., & Fernandes, C. (2023). ‘You Just Treat me like a Human Being’: Using Lived Experience to (Re)imagine Boundary Practices in mental health settings. The British Journal of Social Work, 53(3), 1408–1425. https://doi.org/10.1093/bjsw/bcad044
Sudbery, J. (2002). Key features of therapeutic social work: The use of relationship. Journal of Social Work Practice, 16(2), 149–162. https://doi.org/10.1080/0265053022000033711
Szumer, R. T. O., & Arnold, M. (2023). The ethics of overlapping relationships. Journal of Bioethical Inquiry, 20(2), 181–190. https://doi.org/10.1007/s11673-023-10225-8
Telander, K., Hosek, S. G., Lemos, D., & Jeremie-Brink, G. (2017). “Ballroom itself can either make you or break you” – Black GBT Youths’ psychosocial development in the House Ball Community. Global Public Health, 12(11), 1391–1403. https://doi.org/10.1080/17441692.2017.1293123
Thompson, V. L. S., & Alexander, H. (2006). Therapists’ Race And African American Clients’ Reactions To Therapy. Psychotherapy (Chicago, Ill.), 43(1), 99–110. https://doi.org/10.1037/0033-3204.43.1.99
Toomey, R. B., Ryan, C., Diaz, R. M., Card, N. A., & Russell, S. T. (2010). Gender-Nonconforming Lesbian, Gay, Bisexual, and Transgender Youth: School Victimization and Young Adult Psychosocial Adjustment. Developmental Psychology, 46(6), 1580–1589. https://doi.org/10.1037/a0020705
Toomey, R. B., Ryan, C., Diaz, R. M., & Russell, S. T. (2018). Coping with sexual orientation–related minority stress. Journal of Homosexuality, 65(4), 484–500. https://doi.org/10.1080/00918369.2017.1321888
Tower, K. D. (1994). Consumer-Centered Social Work Practice: Restoring Client Self-determination. Social Work (New York), 39(2), 191–196. https://doi.org/10.1093/sw/39.2.191
Trans Legislation Tracker. (2026). Tracking anti-trans legislation across the United States. Retrieved 3.20.26, from https://translegislation.com/
Tsang, N. M. (2008). Kairos and practice wisdom in social work practice: kairos. European Journal of Social Work, 11(2), 131–143. https://doi.org/10.1080/13691450701357315
Velez, C., Sloan, L., Al-Kaabi, I., Cuddy, A., & Kerrigan, J. (2023). No Sex in Social Work: (the Lack of) Human Sexuality Courses in US Social Work Education. Journal of Human Rights and Social Work, 8(1), 2–13. https://doi.org/10.1007/s41134-022-00230-3
Ward, A., Ruch, G., & Turney, D. (2018). Relationship-Based Social Work, Second Edition: Getting to the Heart of Practice, Edited by Gillian Ruch, Danielle Turney and Adrian Ward. In Relationship-Based Social Work, Second Edition. Jessica Kingsley Publishers.
Warshaw, C. (1989). Limitations of the Medical Model in the Care of Battered Women. Gender & Society, 3(4), 506–517. https://doi.org/10.1177/089124389003004008
Webb, J. M. (2025). Educational cultural visionaries: how BlackQueer adults mentor, embrace, and love on BlackQueer youth. International Journal of Qualitative Studies in Education, 1-14. https://doi.org/10.1080/09518398.2025.2470935
Whitsett, D. P., & Whitsett, D. A. (1996). Anti-Black Racism and Its Consequences: A Self Psychology/Object Relations Perspective. Journal of Analytic Social Work, 3(4), 61–81. https://doi.org/10.1300/J408v03n04_05
Woodcock, R. (2011). Ethical Standards in the NASW Code of Ethics: The Explicit Legal Model, and Beyond. Families in Society, 92(1), 21–27. https://doi.org/10.1606/1044-3894.4052
Wright, A. J. (2021). A practical application of Self Psychology in counseling. Journal of Counselor Preparation and Supervision, 14(4), 13.
